CHAPTER 10
PALM OF HAND
The skin of
the palm is thick and the superficial fascia contains palmaris brevis muscle
across the base of hypothenar eminence.
Deep fascia is thickened to form:
Flexor retinaculum
Palmar aponeurosis
Fibrous flexor sheaths of digits
Flexor retinaculum:
It covers the anterior concave surface of the carpus into
an osseo fibrous carpal tunnel

Attachments:
Medially – pisiform bone and hook of the hamate
Laterally - tubercle of scaphoid and the crest of
trapezium

Palmaris longus tendon
Palmar cutaneous branch of median nerve
Palmar cutaneous branch of ulnar nerve
Superficial palmar branch of radial artery
Ulnar nerve and ulnar vessels
In between superficial and deep
slips on the lateral distal part, flexor carpi radialis tendon passes.

Structures passing deep to flexor retinaculum:
Median nerve
Tendons of flexor digitorum superficialis and
Tendons of flexor digitorum profundus-these two tendons are covered by the common synovial sheath called ulnar bursa
Tendon of flexor policis longus is covered by a synovial sheath called radial bursa
APPLIED ANATOMY:
Carpal tunnel syndrome:
Compression of median nerve in the carpal tunnel by the long continued swelling of synovial sheath is called carpal tunnel syndrome.
Manifestations are:
weakness and wasting of thenar muscles.
Loss of opposition of thumb
Loss of cutaneous sensations of the palmar surface of
lateral 3 ½ digits.
Palmar aponeurosis:
It is thickened deep fascia of palm.
It consists of three
parts:
Central part – thick
Medial part and lateral parts are thin

- Central part is thick and called palmar aponeurosis proper.
- It is triangular in shape
- Apex directed proximally and is continuous with the tendon of palmaris longus.
- Distally, the aponeurosis splits into four digital slips for the medial four fingers.
- Each slip divides into superficial and deep set of fibers
- Superficial slip is continuous with the dermis and blend with superficial transverse ligament of palm.
The deep set fibres divides into two bands which are
continuous with
- deep transverse ligament of palm
- palmar ligaments of meta carpophalangeal joints
- fibrous flexor sheaths of digits
Medial and lateral palmar septa extend dorsally from the
respective margins of the central part of palmar aponeurosis.
APPLIED ANATOMY:
The inflammatory contracture of the palmar aponeurosis is known as Duputren’s contracture.
It manifests as:
- Proximal and middle phalanges are acutely flexed as the palmar fascia is attached to them
- Terminal phalanges remain unaffected
Intrinsic
muscles of Hand:
Thenar muscles are:
- Abductor pollicis brevis
- Flexor pollicis brevis
- Opponens pollicis
- Adductor policis
Hypothenar muscles are:
- Abductor digiti minimi
- Flexor digiti minimi
- Opponens digiti minimi
- Palmaris brevis
- Four lumbrical muscles
- Four palmar interossei
- Four dorsal interossei
Lumbrical Muscles:
Four small muscles resembling the shape of earthworm,
ascaris lumbricoides and hence the name. They are numbered from lateral to
medial side
Origin: From the four tendons of flexor digitorum
profundus. First two lumbricals are unipennate and the other two lumbricals are
bipennate

Insertion: In to the dorsal digital expansion of medial
four fingers
Nerve supply: First and second lumbricals are supplied by
the median nerve.
Third and fourth lumbricals are supplied by the deep branch
of ulnar nerve.
Actions:
They are the ‘link muscles’ connecting the flexor tendons
with the extensor tendons.
Flex the metacarpophalangeal joints and extend the
interphalangeal joints – important for gripping pens, brush etc.
Interosseous Muscles of Hand:
Palmar interossei
Dorsal interossei
Palmar interossei:
Four muscles – all are unipennate
Act as adductors of fingers (REMEMBER AS PAD)
The middle finger is the axis – and it has no adduction.
Origin:
All are unipennate and arise from the medial side of 1st and 2nd meta
carpal bones and 3rd and 4th arise from lateral side of 4th
and 5th meta carpal bones.
Insertion:
Partly attached to the proximal phalanges and partly into
the dorsal digital expansion of digits

Four muscles – all are bipennate
Act as abductors of fingers
As the middle finger is the axis, it has 2 abductors (2
dorsal interossei)
Origin:
All are bipennate and arise from the adjacent sides of the
meta carpal bones.
Insertion:
1st and 2nd dorsal interossei are
inserted into the lateral sides of the proximal phalanges of the index and
middle fingers and into their dorsal digital expansion.
3rd and 4th dorsal interossei are
inserted into the medial sides of the proximal phalanges of the middle and ring
fingers.
Nerve supply: Deep Branch of ulnar nerve.
Superficial Palmar Arch:
It is an arterial arch which lies
beneath the palmar aponeurosis
Formation:
The arch is
formed by the superficial terminal branch of ulnar artery joined on lateral
side by any of the following arteries-
- Superficial palmar branch of radial artery
- Arteria princeps pollicis (principal artery of thumb)
- Arteria radialis indicis (Artery on radial side of index finger)
- Median artery

Branches:
Four palmar digital arteries
One proper digital side to the left finger
Three common digital arteries
Deep palmar arch:
It is
arterial arch which lies deep to oblique head of adductor pollicis. The deep
branch of ulnar nerve accompanies the concavity of the deep palmar arch.
Formation: Formed by the terminal end of radial artery
joining the deep branch of ulnar artery.
Branches:
Three palmar metacarpal arteries
Three perforating arteries
Recurrent branches
Fascial spaces in the palm:
There are fascial lined potential spaces in the palm and the
palmar aspect of the terminal phalanges
They are:
- Mid palmar space
- Thenar space
- Pulp space
Situation: In the palm, deep to long flexor tendons and
lumbrical muscles, lies the fascial spaces limited on each side by the medial
and lateral palmar septa.
Mid palmar space:
Triangular in shape
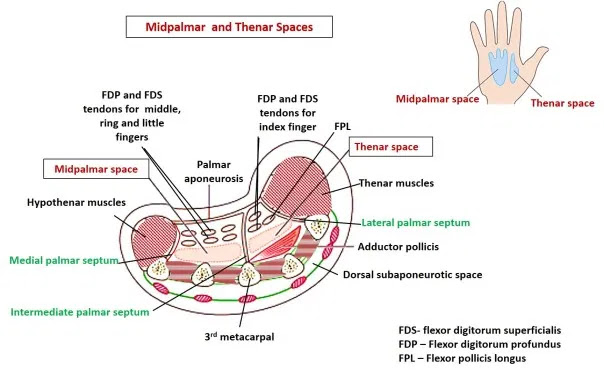
It presents the following boundaries:
Infront: Flexor tendons of little, ring, middle fingers
with their lumbrical muscles ( 3rd and 4th)
Behind: the dense fascia covering the interossei and the
meta carpal bones of 3rd and 4th spaces.
Medially: hypothenar muscles separated by the medial palmar
septum
Laterally: Intermediate fibrous septum

Proximally: the space is closed
Distally: the space extends as diverticula to the webs of
fingers along the fascial sheaths of 3rd and 4th
lumbrical muscles.
Thenar space:
Triangular in shape
It presents the following boundaries :
Infront:
Muscles of thenar eminence
Flexor tendon of index finger
1st and 2nd lumbrical muscles

Behind: Adductor pollicis muscles
Medial Side: Intermediate palmar septum
Laterally: Flexor pollicis longus tendon
Proximally: The space is closed
Distally: it is continuous as diverticula to the webs of
fingers along 1st and 2nd lumbrical muscles.
Pulp Spaces:
The spaces
intervening between the palmar slum and distal phalanges of all digits of the
hand are called pulp spaces.
They lie distal to the fibrous sheaths of flexor tendons.
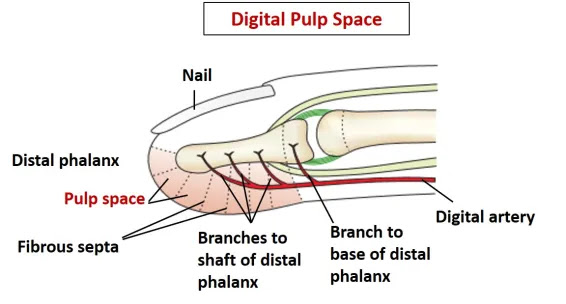
In each pulp space, the skin is connected by the fibrous
septa to the periosteum of the distal phalanx and is divided into many
compartments.
The digital arteries for the distal fourth fifth of the distal
phalanx pass through these septa.
Applied Anatomy:
Pus in the thenar space and mid palmar space can be drained
surgically by splitting the corresponding web spaces and exploring the
lumbrical canal.
Infection of the pulp space is called whitlow. It can cause
avascular necrose of the distal part of the phalanges if untreated. It can be
drained by the lateral incision which opens all the inter septal compartment.


Comments
Post a Comment